How does malaria impact education and gender equality? Evidence from Rwanda
Introduction
The Covid-19 pandemic highlighted the negative socioeconomic impacts associated with the disease. However, malaria has impacted the health and economic outcomes of people in the tropics for several millennia. The disease is endemic and life-threatening in more than 94 countries, with Sub-Saharan Africa accounting for the highest concentration of countries at risk. In 2018 alone, 228 million cases of malaria infection and 405,000 malaria-related deaths were recorded. About 94% of these deaths were recorded in Africa.
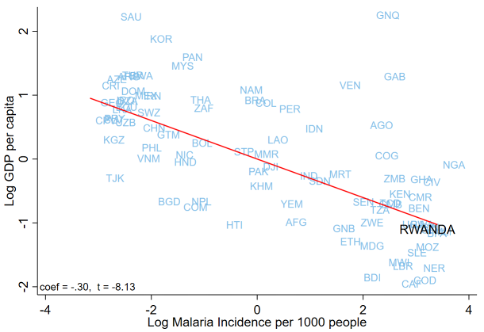
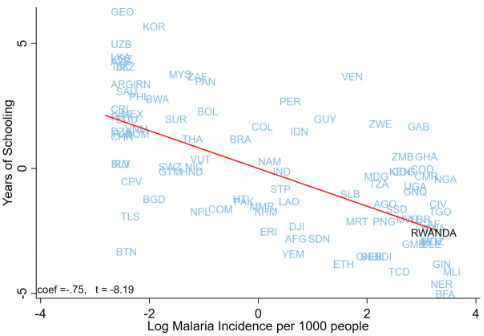
The extended socioeconomic effects of malaria manifest in various forms, one of which is a reduction in educational attainment and subsequent human capital accumulation. Aside from the worrying morbidity and mortality rates associated with malaria, available evidence suggests that the disease has a significant long-run impact on economic development, with low productivity and human capital accumulation as likely operative channels. For instance, Figure 1 panel A shows a negative cross-country association between malaria incidence and income per capita. In other words, countries with high malaria burdens tend to be poor. Panel B of the same figure also shows the association between malaria incidence and average years of schooling across countries. Again, we observe a negative relationship between malaria and educational attainment across countries.
Figure 1: Malaria, Income, and Educational Attainment
Panel A: Malaria and Income
Panel B: Malaria and Educational Attainment
In our working paper, Malaria and Human Capital Accumulation,[1] we use unique administrative data from Rwanda to provide evidence on the effects of malaria on education and how the disease continues to widen gender gaps. There are at least four channels through which malaria affects education in the tropics. The first relates to fetal and cognitive development. In-utero exposure to malaria is often associated with anemia and other health-related issues, which can ultimately impair the physical and cognitive development of the child. As a result, early-life exposure to malaria can have negative consequences on the cognitive performance of children in school, resulting in low educational attainment.
Second, high incidence of malaria infections affects school attendance as infected students spend more time either at home or in health facilities undergoing treatment. In some cases, school-aged children, particularly girls, stay home to care for family members with malaria. Such frequent interruptions in schooling resulting from malaria can hinder learning and grade progression, ultimately leading to students dropping out of school.
Third, in many developing countries, access to health insurance is limited. Most households finance health expenditures themselves. This has severe consequences for non-health expenditures, such as education, as many of these households face a binding constraint on income. In other words, malaria can induce income reallocation from education to health, thereby reducing household investments in education.
The last channel relates to the expected returns to schooling. The extant literature documents evidence of a negative impact of malaria on labor productivity and, hence, wages. This means malaria is likely to reduce the expected returns to schooling, thus lowering the households’ incentive to educate their children.
Malaria in Rwanda
Rwanda’s geoclimatic condition is suitable for malaria transmission throughout the year although with fluctuations tied to seasonal temperature variations. The country is located on highlands just below the equator and it receives year-round precipitation, providing an optimal environment for the reproduction of the mosquito, Anopheles gambiae, responsible for malaria transmission. This inherent suitability for malaria transmission puts the entire population of the country potentially at risk.
As in other countries in the tropics, Rwanda is facing increasing challenges from malaria, which is among the leading causes of morbidity and mortality. Data from the Rwanda Health Management System (HMIS) shows that between 2012 and 2017, Rwanda experienced a quadrupling malaria incidence rate from 93 per 1,000 in 2012 to 418 per 1,000 in 2017. This increase was observed in all districts, including those where the disease had previously been eradicated. In addition, individuals tested positive for malaria increased from 34% to 42% among the total sample population between 2012 and 2015[2]. In the same period, malaria morbidity increased from 5.9% to 21.5%.
Among malaria parasites, the endemic one in Rwanda is Plasmodium Falciparum. The prevalence of the parasite depends largely on the malaria ecology, i.e. the conditions suitable for the survival of the malaria parasite. Malaria transmission suitability is, however largely determined by climatic conditions, key among which is temperature. Thus, changing climatic conditions influence the survival and spread of malaria across locations and time.
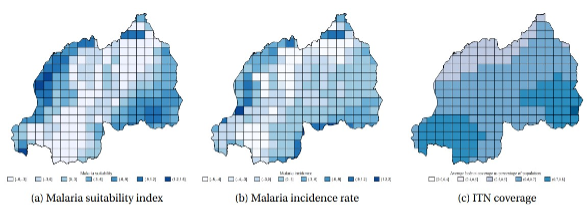
Figure 1 shows the distribution of malaria suitability, incidence, and Insecticide Treated Nets (ITN) coverage in Rwanda. Panel (a) provides malaria transmission suitability in each grid cell averaged across years and standardized with a mean 0 and a standard deviation of 1. Panel (b) plots the malaria incidence rate averaged across years for each grid cell. The incidence rate is standardized with a mean 0 and a standard deviation of 1. Panel (c) plots the average insecticide treated bed-net coverage per grid cell.
Figure 2: Malaria suitability, incidence, and ITN coverage
Malaria prevalence and educational outcome
The study examined the relationship between malaria prevalence and test scores of students who sat for grade six exams between 2012 and 2017 in Rwanda. School location was used to measure students’ predicted exposure to malaria, which was constructed relying on the relationship between weather and malaria transmission. A location’s suitability for malaria transmission is dependent on temperature and precipitation, which determine the mosquito’s reproduction and activity, the malaria parasite’s survival rate, and duration of the sporogonic cycle.
Regression results presented in Figure 3 show that a one-standard deviation increase in malaria transmission suitability is associated with a 0.31, 0.3 and 0.29 standard deviation decrease in the aggregate score, and in the score of STEM subjects and non-STEM subjects respectively. [3] These results indicate that, despite considerable mitigation efforts, malaria continues to exert significant effects. Existing literature shows that childhood education attainment determines later-in-life achievements. Thus, the reduction in test scores as a consequence of malaria will limit human capital accumulation and could exacerbate existing inequalities in education, disadvantaging already vulnerable populations.
Figure 3: Relationship between malaria transmission suitability and test scores
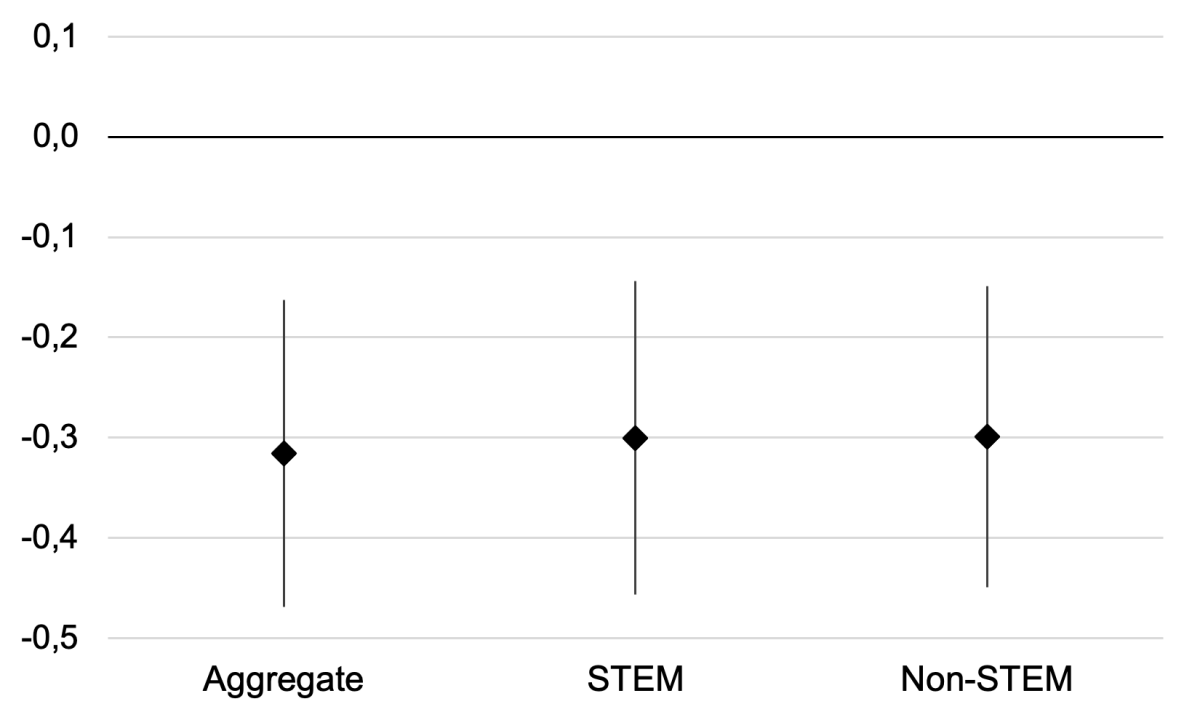
Note: Diamonds show estimated coefficients and vertical lines show 95% confidence interval.
The timing and location of an exam also affects student test scores. Students sitting for an exam in a location and in a month that are relatively more suitable for malaria transmission score less than their peers writing an exam in a place and at a time less favorable for malaria transmission.
Malaria and the educational gender gap
Evidence from the literature points to gender inequalities in people at risk of malaria and its associated effects. Even though, biologically, pregnant women and children are more vulnerable to malaria, socioeconomic factors increase the risks for women. The inequalities in resource allocation, intra-household decision-making, and labor allocation are among the primary drivers of gender gaps in the effects of malaria.
Many female-headed households in Sub-Saharan Africa (SSA) are low-income earners. This limits their ability to invest in malaria prevention strategies such as treated nets, adequate nutritional intake, quality housing, and even their ability to pay for malaria medications. In addition, sociocultural norms in most developing countries influence decision-making in households. For instance, women are often not involved in decision-making on various issues, including health care. In some communities, women are expected to seek their husbands' permission to access healthcare.
In the context of this study, however, the primary source of malaria-induced gender differences in students' performance relates to labor allocation at the household level, where women and school-aged girls bear a greater burden of taking care of sick household members. For example, when a household member falls ill with malaria, school-aged girls are likely to temporarily drop out from school to care for the sick person, while school-aged boys in the family continue to attend school.
Thus, malaria lowers school performance for girls relative to boys. Specifically, a one-standard deviation increase in a school’s location in terms of malaria transmission suitability reduces girls' test scores by about 0.038 standard deviations relative to boys. We further find that the gap is even higher for science subjects (STEM) test scores than non-science (non-STEM) test scores, which are 0.045 and 0.031 standard deviations, respectively.
Mitigation and treatment: access to insecticide-treated bed nets (ITN) and health care
The main malaria control strategy recommended by the World Health Organization (WHO) is the use of ITNs by households in malaria endemic areas. As a result, significant public and donor funding resources have been spent on the distribution of ITNs to households to limit the incidence of malaria, particularly among pregnant women and children, who are the most at-risk population. Here we ask, how does access to ITN mitigate the effects of malaria on student performance? By splitting the study area into three suitability zones (low, medium, and high), each containing one-third of the malaria suitability distribution, we found that in high malaria zones, students in places with high uptake of ITNs perform better than their counterparts in places with low uptake. In medium malaria suitability zones, we again observed a positive effect, albeit the estimates are barely significant statistically, even at a 10% error level. For the low malaria zones, however, we do not observe a significant difference in performance between students in areas with high ITN uptake and those in areas with low uptake. From this, we conclude that ITN is an effective channel in reducing the effects of malaria on student performance, particularly in high malaria zones.
We further evaluate the importance of access to health care in the relationship between malaria and test scores. Using geodata on the location of health facilities and schools in Rwanda, we estimate the straight-line distance between each school and the nearest health facility. The study shows that the effects of malaria suitability on students' test scores are almost zero and statistically insignificant if they are within 6km of a health facility. However, the effect increases (negatively) in places within 6-9 km and 9-15km from a health facility, relative to the reference group, which is 0-3km. This suggests that malaria affects student performance in places with constrained access to health care, and where students have poor access to treatment when infected.
Transmission channels
Apart from the obvious health channel, we explore two potential channels through which malaria affects student performance. These include school absenteeism and household spending. The study finds a negative association between malaria and the probability of a student attending school. Specifically, a one-standard deviation increase in the malaria suitability index is associated with a 9.5 percentage point increase in absenteeism. Relative to the sample mean, this represents a 15% increase in absenteeism rate. This effect is substantial and plausibly underlines the effects on test scores observed in earlier sections.
How does malaria affect household spending? In the absence of health insurance, malaria prevalence, like most diseases, is expected to increase household health spending. Other things being equal, this may negatively impact non-health expenditures, such as spending on education. The study shows a statistically significant effect of malaria on the log of total household health expenditure. Specifically, a one-standard deviation increase in malaria suitability is associated with a 1,155 Rwandan Franc increase in health spending, which is a 16% increase relative to the mean.
Conclusion
In our study, we examined the effects of malaria on human capital accumulation leveraging administrative data on test scores of more than a million primary school students in a high-stake national exam in Rwanda and linked these with granular spatial data on malaria ecology between 2012 and 2017. We found that exposure to malaria significantly reduces students’ test scores. There is also evidence that malaria widens the gender gap in student performance, as the effect on the test scores of girls is relatively higher than boys. In examining the possible causes for this, we found absenteeism is the most likely channel: infected children often have to stay home or in a hospital to undergo treatment, or, in the case of girl-children, have to care for family members.
Our results have relevant policy implications. To prevent the short-term effect of malaria on students’ educational performance, a well-timed prevention campaign such as access to prophylaxis, mosquito-control programs, and increasing use of new and effective ITNs could be useful. In addition, the results emphasize the need to acknowledge the additional burden of malaria on girls. Efforts to close the gender gap should consider the unequal effects of malaria.
References
Bleakley, H. (2010). Malaria eradication in the Americas: A retrospective analysis of childhood exposure; American Economic Journal: Applied Economics, 2(2):1–45.
Cutler, D., Fung, W., Kremer, M., Singhal, M., and Vogl, T. (2010). Early-life malaria exposure and adult outcomes: Evidence from malaria eradication in India; American Economic Journal: Applied Economics, 2(2):72–94.
Duffy, P. E. and Desowitz, R. S. (2001). Pregnancy malaria throughout history: dangerous labors. In Malaria in Pregnancy, pages 17–43. CRC Press.
Rwanda Biomedical Center (2017): Rwanda Malaria Strategic Plan (2013-2018). Mid-Term Review. September 2016, Kigali
UNDP (2015). Gender and Malaria; Technical report, United Nations Development Program.
WHO (2019). World Malaria Report, 2019
[1] UNU-WIDER working paper; forthcoming.
[2] Those statistics have been compiled by the Rwanda Biomedical Center (RBC) based on Rwanda Demographic and Health Surveys (RDHS, 2014/15) and Rwanda Health Information Management System (HMIS).
[3] The STEM is a common abbreviated term used to stand for Science, Technology, Engineering and Mathematics while non-STEM refers mostly to social sciences subjects such as languages.
Download article
Post a commentary
This comment facility is intended for considered commentaries to stimulate substantive debate. Comments may be screened by an editor before they appear online. To comment one must be registered and logged in.
This comment facility is intended for considered commentaries to stimulate substantive debate. Comments may be screened by an editor before they appear online. Please view "Submitting a commentary" for more information.